

Abstract
Background Hypomethylating agent (HMA) therapy represents the standard of care for patients with higher risk myelodysplastic syndromes (MDS) although only 50% of patients respond to treatment. Recent evidence from molecular profiling through next-generation sequencing (NGS) in myeloid diseases has been conflicting as to the value of somatic mutations as a biomarker for response to HMA. In particular, there have been conflicting data on response rates and outcomes in TP53 mutant (MT) MDS and acute myeloid leukemia (AML) based on azacitidine versus decitabine (Welch et al., NEJM 2016; Garcia-Manero et al., NEJM 2017). However, the TP53 mutant cohorts in these studies were small (median 23 patients, range 13-39) and heterogeneous based on treatment status (treatment naïve versus relapse/refractory). Therefore, our goal was to characterize outcomes of TP53 mutant MDS patients who received frontline HMA therapy.
Patients and MethodsTP53 MT MDS and oligoblastic AML (20-30% blasts) cases were retrospectively identified from the Moffitt Cancer Center MDS database. All patients had NGS of TP53 and up to 53 additional genes performed prior to the initiation of HMA. The lower limit of VAF detection was set at 5% and the minimum depth of coverage at each position was 500X. Clinical variables and outcomes of MDS patients were characterized at the time of sample procurement. Fisher's exact tests were used for comparative analyses. Kaplan-Meier curves were used to estimate overall survival (OS) and analyzed from the date of HMA initiation. Response rates and outcomes of TP53 MT patients were compared to a cohort of wildtype (WT) patients (n=63).
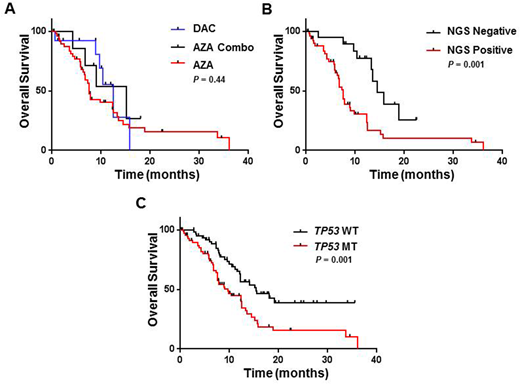
Results From May 2013 to May 2018, a total of 71 patients with TP53 mutant MDS were identified with a median age of 68 years (39-82) and male predominance (66%). Fourteen patients (20%) had multiple mutations in TP53. Of the cohort, 82% of patients (n=58) were treated with azacitidine (88% (n=51) with AZA monotherapy; 12% (n=7) with AZA in combination (2 pts with lenalidomide and 5 pts with investigational agents)) with 18% (n=13) receiving decitabine. The median # of HMA cycles was 4 (range 1-33). Thirteen pts (18%) proceeded to allogeneic hematopoietic stem cell transplant (HSCT). Of the cohort, 18% (n=13) obtained complete remission (CR) with 39% (n=28) overall response rate (ORR). There was no difference in CR or ORR in pts treated with AZA vs DAC (P=0.24 and P=0.2, respectively). At a median follow up 20 months, the median OS of the entire cohort was 9.7 months. There was no difference in median OS between AZA vs AZA combo vs DAC (7.6 vs 15.2 vs 12.5 months; P = 0.44; Figure 1A). TP53 variant allele frequency (VAF > 20% vs ≤ 20%) was not predictive of outcomes to HMA (7.8 vs 10.4 months, P = 0.36).
However, TP53 MT patients who had clonal response to HMA (i.e. VAF < 5%; n=19 (27%)) had improved OS (14.5 vs 7.5 months; HR 0.33, 95% CI 0.18 to 0.59; P = 0.001; Figure 1B). In multivariable analysis incorporating age, revised international prognostic scoring system (IPSS-R) category, HSCT status, or type of HMA, TP53 clonal clearance remained an independent covariate for improved OS (HR 0.34, 95% CI 0.16 to 0.72; P = 0.005). Pts who underwent HSCT (n=13) had a trend for improved OS (14.5 months vs 7.9 months; P = 0.09). Notably in transplanted pts who had serial TP53 NGS (n=7), pts who achieved a VAF < 5% had significant improved OS (16.3 months vs 8.9 months; P=0.03). Compared to higher risk MDS/AML TP53 WT patients treated with HMA, there was no difference in CR (18% vs 14% (P = 0.64) or ORR rates (39% vs 40%). In contrast, TP53 MT patients had significantly inferior OS with HMA therapy (9.7 vs 15.4 months; HR 2.14, 95% CI 1.32. to 3.27; P = 0.001; Figure 1C).
Conclusion In this large cohort of higher risk MDS and oligoblastic AML pts who received frontline HMA therapy, TP53 MT patients have significantly inferior OS with no significant differences in response rates or outcomes by HMA. TP53 MT patients who achieve maximum clonal suppression with HMA treatment (i.e. VAF < 5%) have improved OS as well as improved outcome with HSCT. Novel therapy targeting TP53 mutation is needed to improve outcomes.
Sallman:Celgene: Research Funding, Speakers Bureau. Sweet:Agios: Consultancy; Jazz: Speakers Bureau; Astellas: Consultancy; Phizer: Consultancy; Phizer: Consultancy; Astellas: Consultancy; Jazz: Speakers Bureau; Celgene: Honoraria, Speakers Bureau; Novartis: Consultancy, Honoraria, Speakers Bureau; Novartis: Consultancy, Honoraria, Speakers Bureau; Agios: Consultancy; BMS: Honoraria; Celgene: Honoraria, Speakers Bureau; BMS: Honoraria. List:Celgene: Research Funding. Komrokji:Novartis: Honoraria, Speakers Bureau; Celgene: Honoraria, Research Funding; Novartis: Honoraria, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; Celgene: Honoraria, Research Funding; Novartis: Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal